Introduction
While the title is somewhat "tongue in cheek," I find it interesting to consider how one could "learn Medicine" in the shortest amount of time as possible. Whenever I am tasked with learning something complex, I am always guided to do two things:
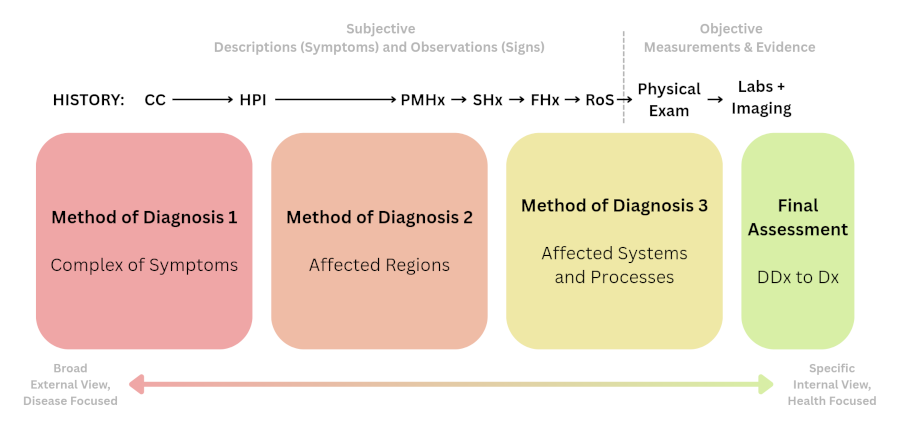
Method of Diagnosis #1: Complex of Symptoms
The first method that comes to mind is sometimes known as a “complex of symptoms.” I imagine that it is what most clinicians do immediately upon interacting with a patient: They think of what ailment(s) could be associated with the set of symptoms that they have described, starting with the most common ones and moving on to the more obscure ones as the possibilities are carefully ruled out. Although, to do this effectively requires a strong understanding of Pathology, an awareness of many different types of diseases and why the particular symptoms of each of them appear (i.e: their pathogenesis).Method of Diagnosis #2: Affected Region(s)
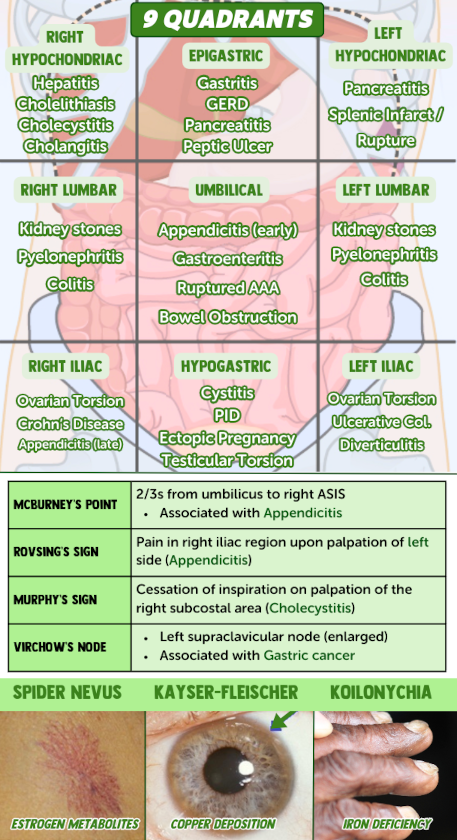
I will refer to the next method of diagnosis as "affected region(s)." It usually coincides with the next part of history taking, the History of Present Illness (HPI). The "elements" of the HPI are questions that help to uncover the nature of the symptoms that accompany their CC, like pain. We should not follow a script. But if we need a guideline for the types of questions to ask, it could be summarized through various acronyms/mnemonics, such as SOCRATES, OPQRST, or OLD CARTS. To go with the latter:| Onset | When did it appear? Did it come on suddenly or gradually? Was there anything specific that triggered it? |
| Location | Where do you feel it? Does it move around or stay in place? Is it concentrated in a given area or is it spread out? |
| Duration | How long does it last? Does it come and go, or is it constant? |
| Character | What type of sensation is it (e.g.: pressure, tingling, burning, throbbing, etc.)? |
| Aggravating factors | Is there anything that makes it feel worse? |
| Relieving factors | Is there anything that makes it feel better? |
| Timing | Does it follow a pattern (e.g.: appearing at a particular time of day)? |
| Severity | How intense is it on a scale of 1 to 10? If it has happened before, is it worse than any past episodes? |
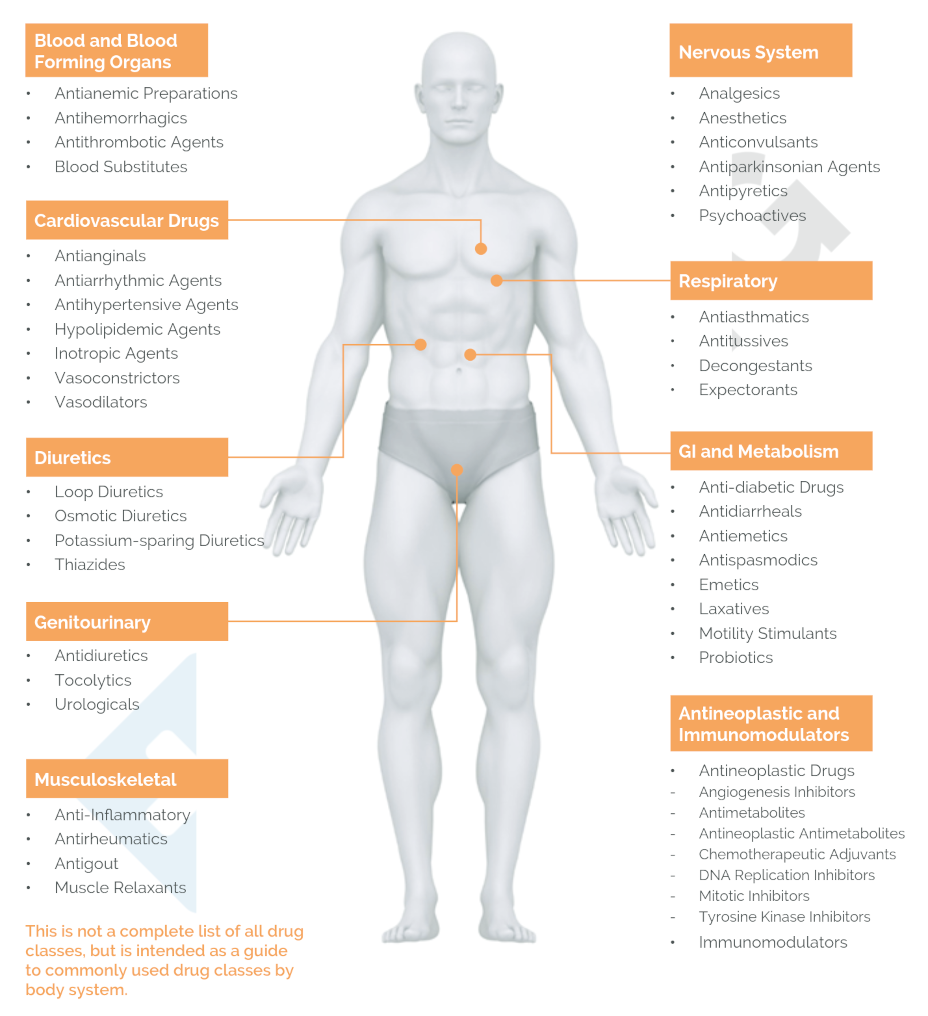
Method of Diagnosis #3: Affected System(s) and Process(es)
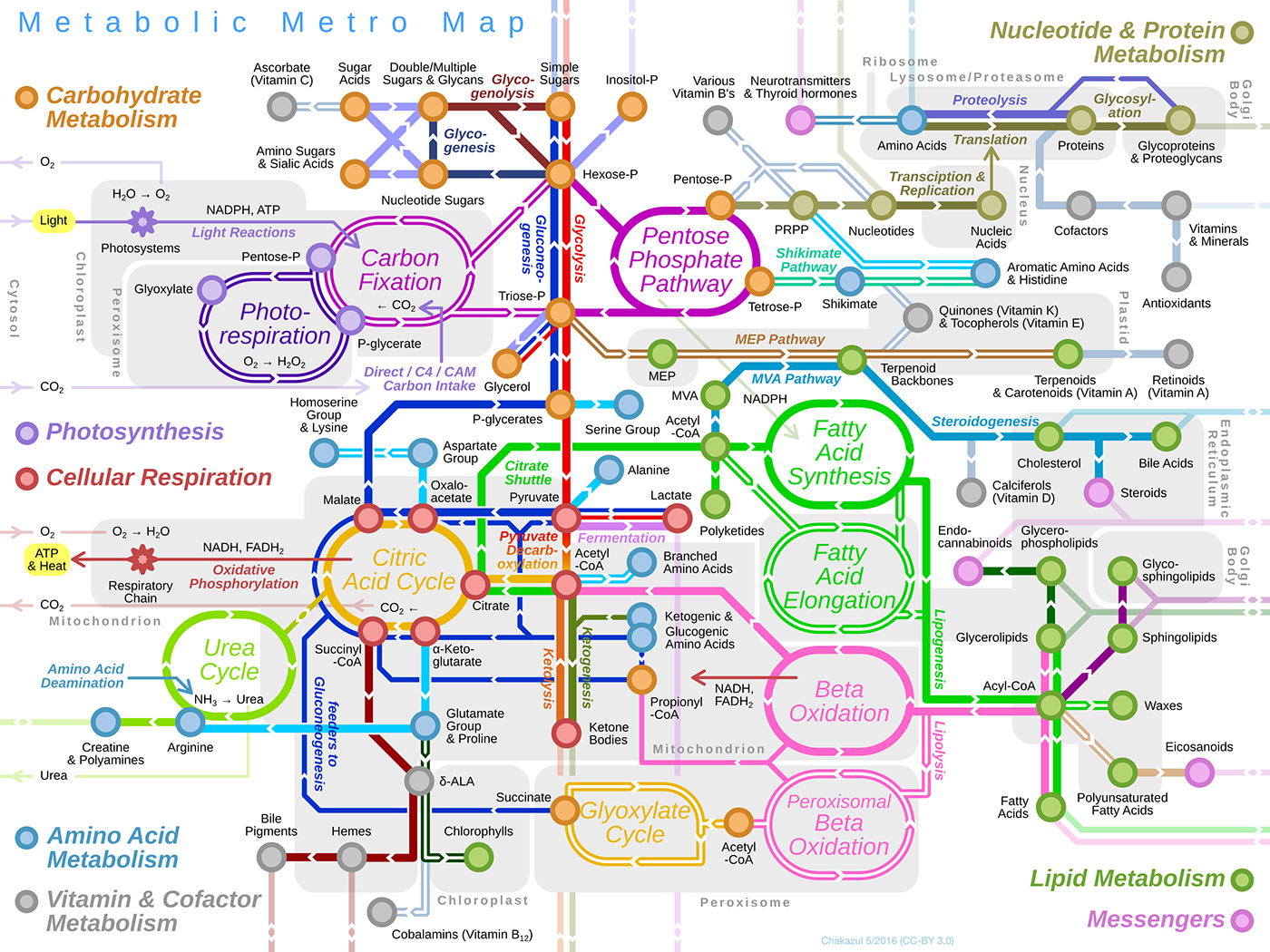
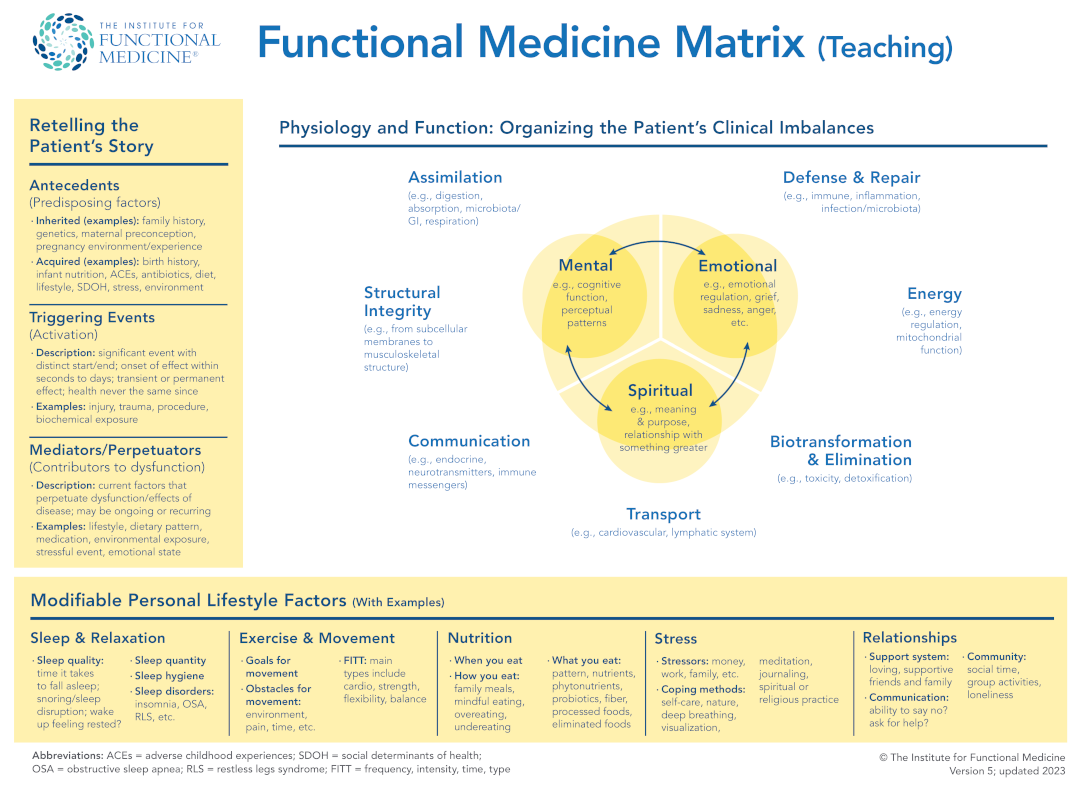
The final method of forming a diagnosis that we will cover here could be called "affected system(s) and process(es)." It requires a strong understanding of Physiology (and the Microbiology, Biochemistry, and Pharmacology related to it). It exists in complement to the previous two methods of diagnosis that we've already mentioned. While it might seem complex, we will try to simplify it by showing some relationships that will allow us to sort out a huge amount of information into a smaller number of useful categories.| General Bodily Function(s) | Organ System |
|---|---|
| Skeletal | |
| Muscular | |
| Integumentary | |
| Nervous | |
| Endocrine | |
| Cardiovascular | |
| Lymphatic | |
| Respiratory | |
| Digestive | |
| Urinary | |
| Reproductive | |
| Texture and Color of Menstrual Blood | (with examples of risk factors in parentheses) |
|---|---|
| excess estrogen, related to symptoms of PMS | |
| low progesterone, related to symptoms of Perimenopause (perhaps trouble with infertility) | |
| low estrogen, related to symptoms of Menopause (perhaps fatigue, a risk for bone fracture) | |
| relatively balanced hormones |
The Three Methods of Diagnosis are Inherent to History Taking
After talking briefly about the CC and HPI, we've covered three more parts of the history with considerable depth: the PMHx, the SHx, and the FHx.| Ideas | What do they think is happening? |
| Concerns | Do they have any specific concerns (e.g.: afraid of having a terminal illness)? |
| Expectations | What are they hoping to achieve or receive? |
| RoS Category | Symptom Examples |
|---|---|
| Constitutional | malaise, weight loss, fever |
| Eyes | vision changes, double vision, eye pain |
| Ear-Nose-Throat (ENT) | ear pain, sinus pain, sore throat |
| Cardiovascular | chest pain, palpitations |
| Respiratory | shortness of breath, wheezing |
| GastroIntestinal (GI) | abdominal pain, nausea, constipation, diarrhea, vomiting |
| GenitoUrinary (GU) | pain with urination, urinary urgency, vaginal discharge |
| MusculoSKeletal (MSK) | weakness, joint stiffness, joint swelling |
| Integumentary | rash, hives, blisters, bruising |
| Neurological | headache, numbness, pins and needles |
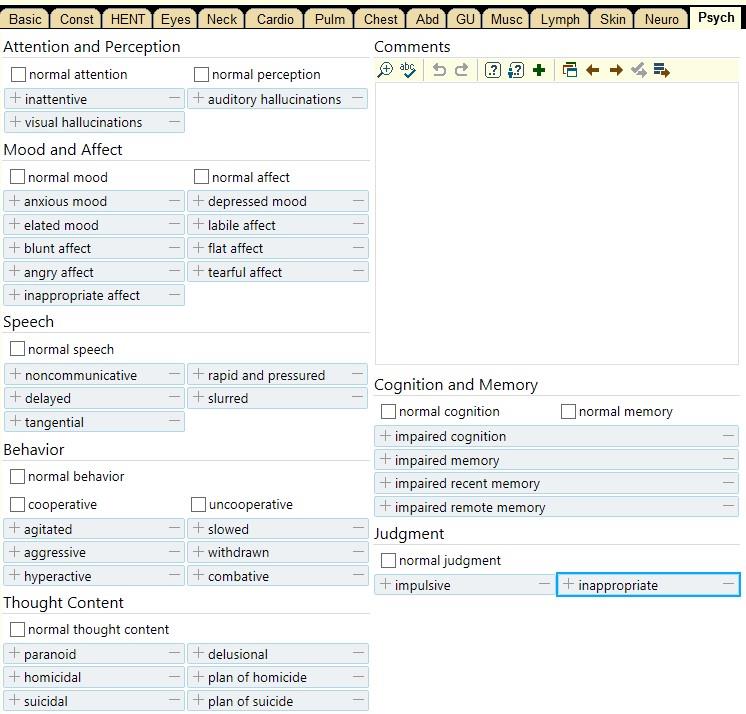
| Psychiatric | depressed, suicidal, homicidal |
| Endocrine | fatigue, cold or heat intolerance, excessive thirst |
| Hematology | abnormal bruising, bleeding gums |
| Allergy and Immunology | swollen glands, hives |
| Constitutional | Eyes | ENT | Cardiovascular | Respiratory |
|---|---|---|---|---|
| [ ] fever/chills [ ] nausea [ ] vomiting × ____ [ ] fatigue [ ] general weakness [ ] excessive sweating (diaphoresis) [ ] night sweats [ ] changes in weight |
[ ] itching [ ] tearing [ ] corrective lenses [ ] blurriness [ ] discharge |
[ ] hearing loss [ ] ear ringing (tinnitus) [ ] spinning (vertigo) [ ] itching [ ] runny nose (rhinorrhea) [ ] allergy [ ] stuffiness [ ] hoarseness [ ] sneezing [ ] nose bleed (epistaxis) [ ] sore throat [ ] neck pain [ ] swollen lymph nodes [ ] bleeding in mouth/throat |
[ ] chest pain [ ] heart murmurs [ ] heartbeat palpitations [ ] shortness of breath lying down (orthopnea) [ ] cramping in extremities (claudication) [ ] awakened by shortness of breath (PND) [ ] leg swelling (edema) [ ] difficulty breathing during activity (DOE) |
[ ] cough [ ] asthma [ ] shortness of breath [ ] pain on inspiration [ ] wheezing [ ] bloody mucus (hemoptysis) [ ] clubbing of fingers [ ] sputum production - color / quantity / smell |
| Gastrointestinal | Genitourinary | Musculoskeletal | Integumentary | Neurological |
| [ ] indigestion [ ] difficulty swallowing (dysphagia) [ ] diarrhea [ ] constipation [ ] yellow skin (from jaundice) [ ] abdominal pain [ ] bleeding, oral or anal [ ] changes in bowel movements (freq., color, blood) |
[ ] urgency [ ] excessive urine (polyuria) [ ] painful urination (dysuria) [ ] waking up to urinate (nocturia) [ ] lesions [ ] blood in urine (hematuria) [ ] discharge [ ] incontinence Last Menstrual Period - timing, regularity, number of days, flow, pain Total number of pregnancies (gravidity) ____ Number of births after 20 weeks (parity) ____ [ ] painful intercourse (dyspareunia) [ ] pregnant |
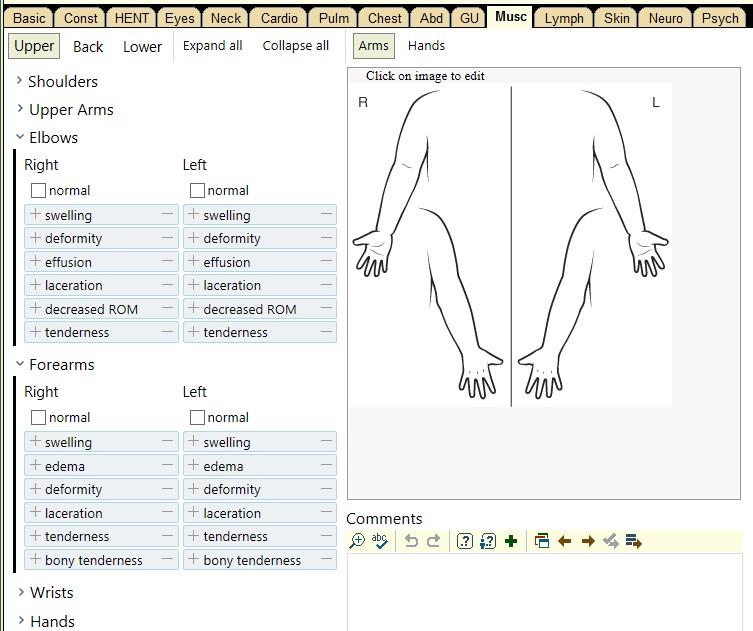
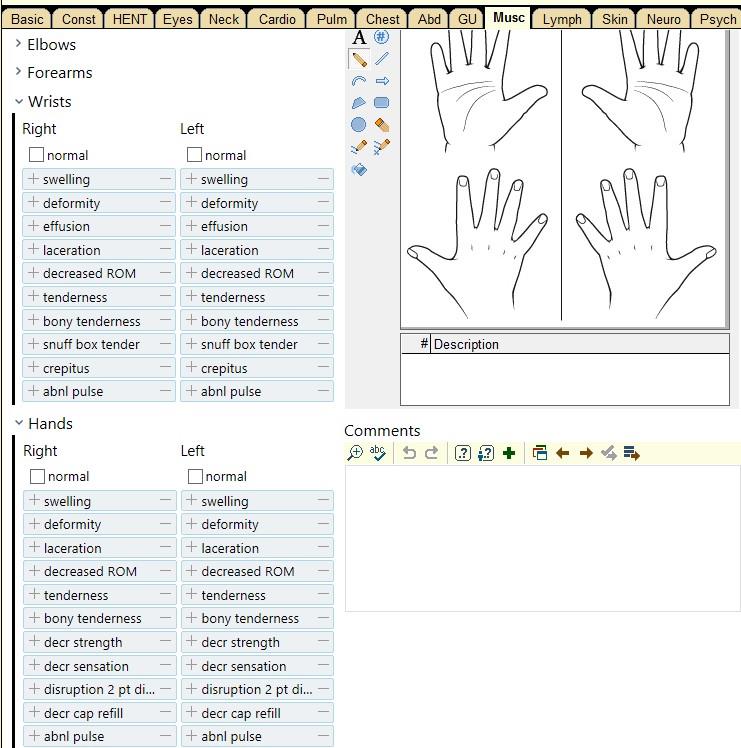
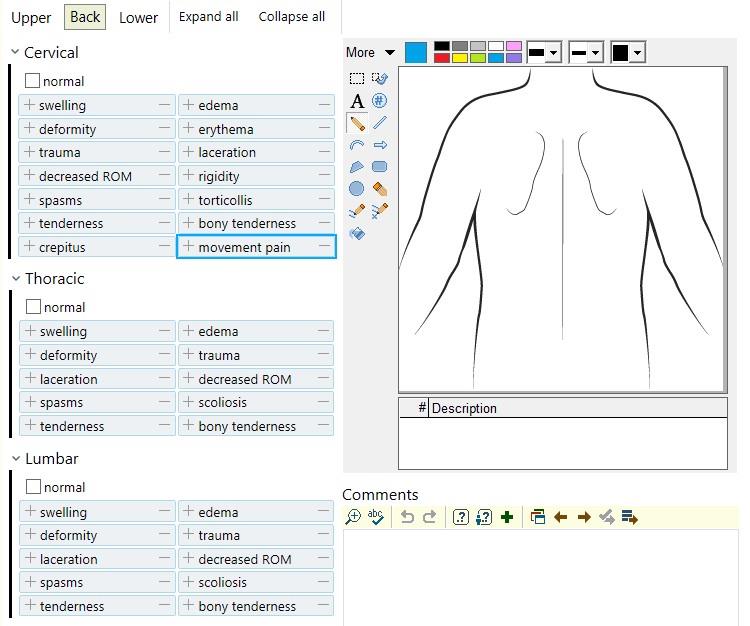
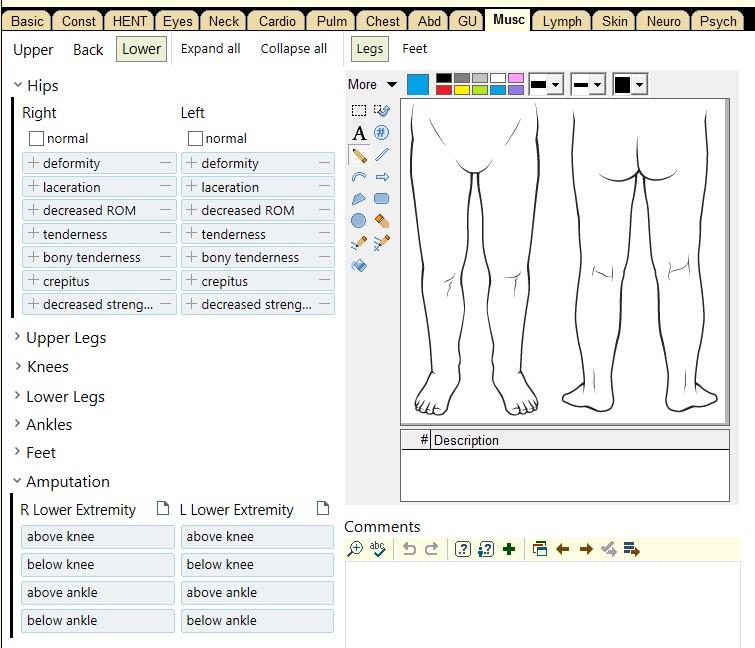
[ ] pain [ ] redness [ ] swelling [ ] joint pain (arthralgia) [ ] normal range of motion [ ] instability |
[ ] itching [ ] rashes [ ] lumps [ ] sores [ ] insect bites [ ] blue skin (cyanosis) |
[ ] fainting (syncope) [ ] slurring of speech [ ] weakness in specific body part (focal weakness) [ ] neck stiffness [ ] decreasing sensation [ ] numbness [ ] tingling [ ] head trauma [ ] loss of consciousness [ ] headache [ ] confusion [ ] lightheadedness (pre-syncope) [ ] changes in vision |
| Psychiatric | Endocrine | Hematology | Allergy / Immune | |
| [ ] stress [ ] anxiety [ ] depression [ ] memory deficits [ ] mood changes |
[ ] breast skin changes [ ] nipple discharge / bleeding [ ] breast pain [ ] breast masses / lumps |
[ ] bruising [ ] small blood spots (petechiae) [ ] large blood spots (purpura) [ ] fatigue (from anemia) |
[ ] swollen glands [ ] hives [ ] sneezing [ ] watery eyes (epiphora) |
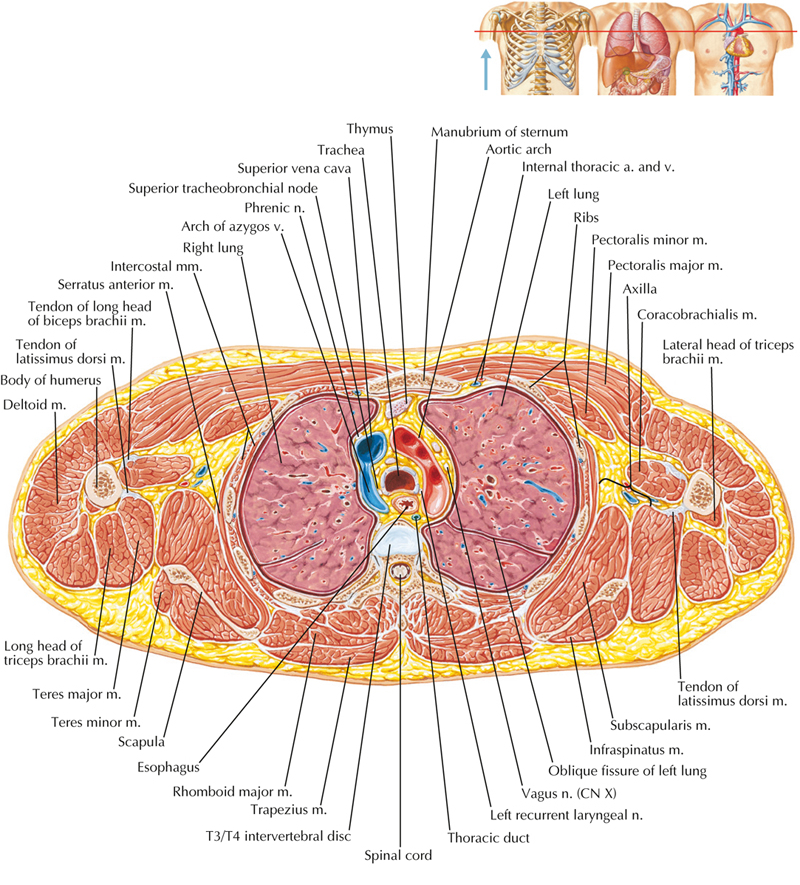
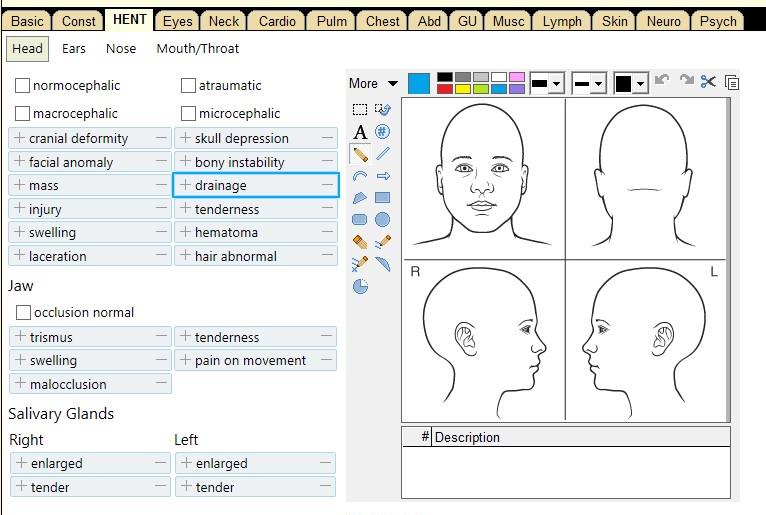
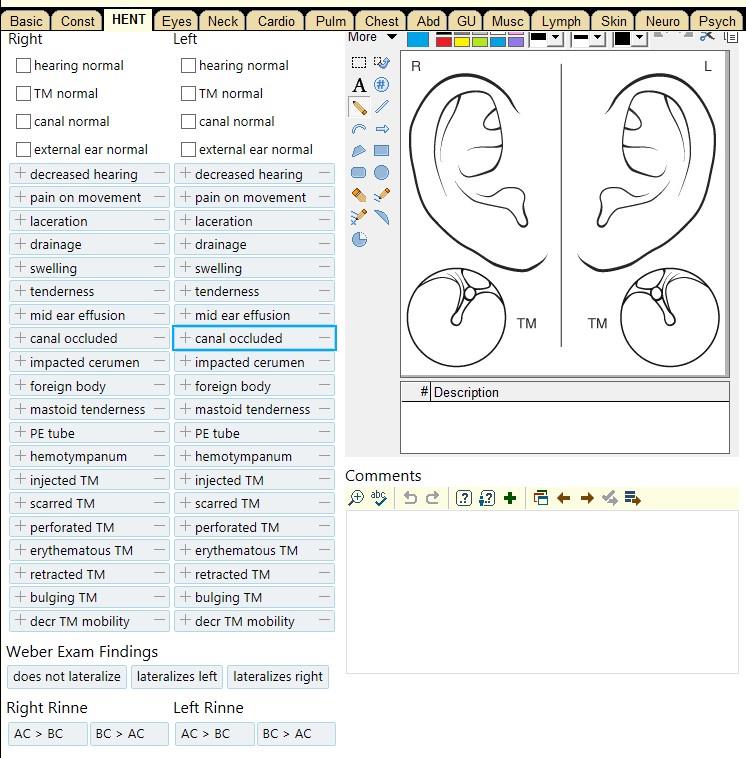
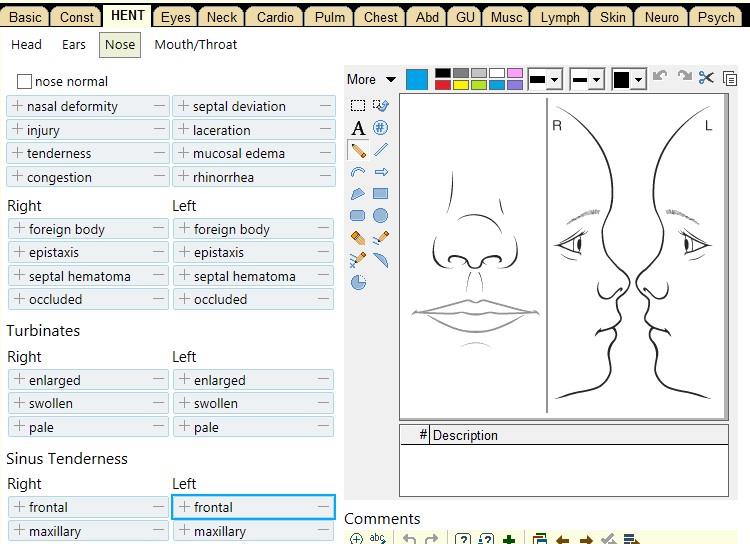
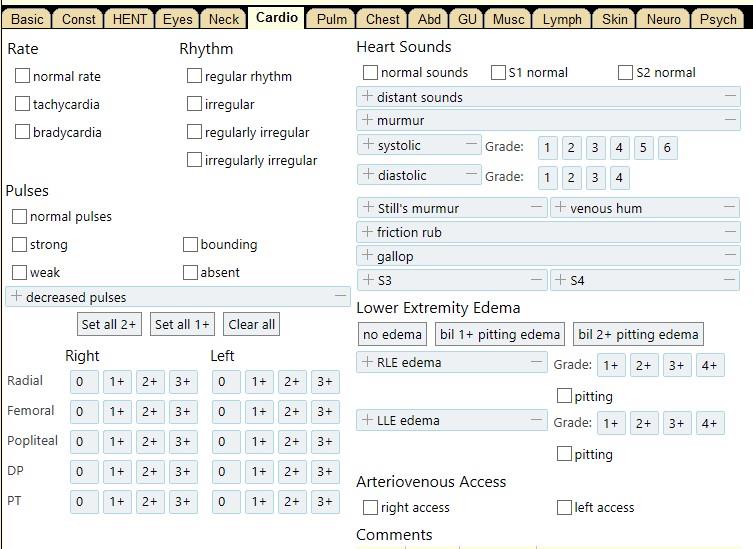
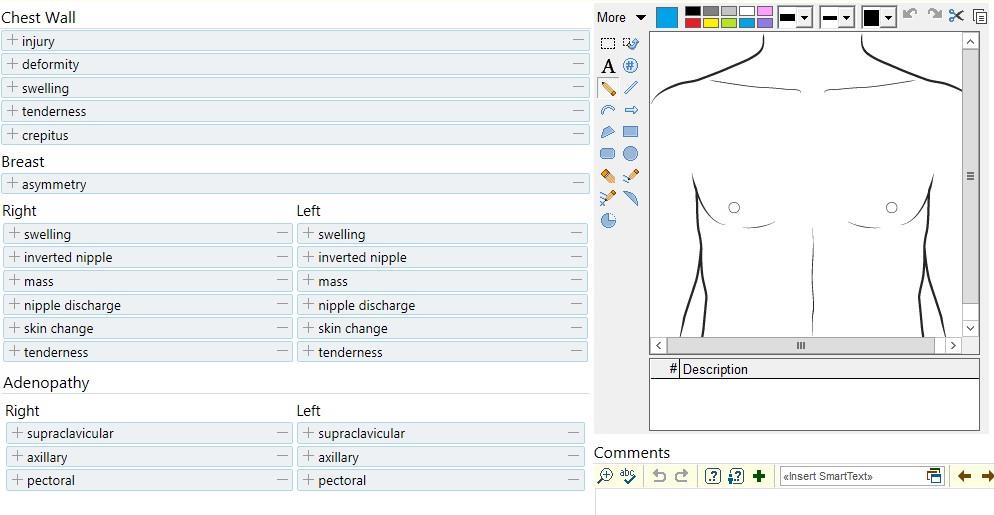
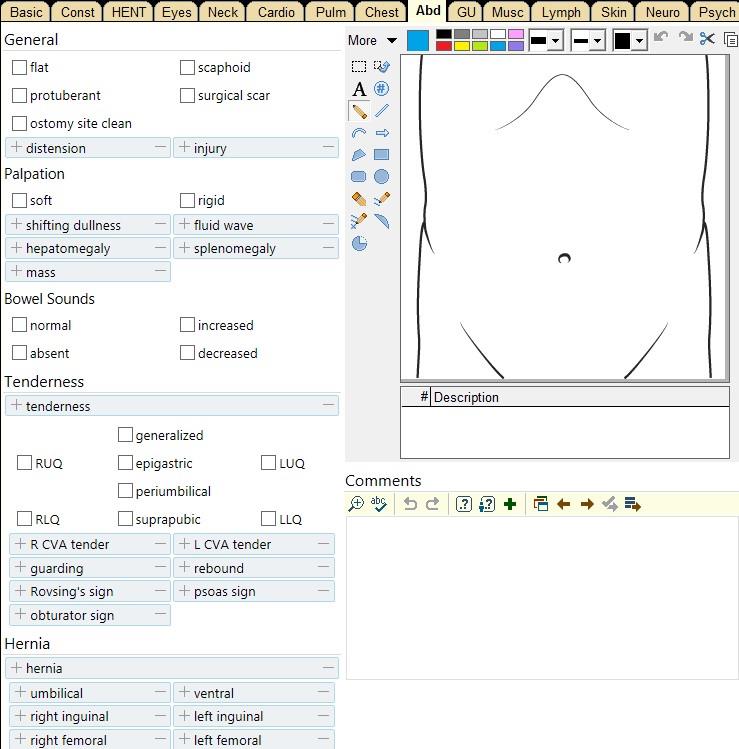
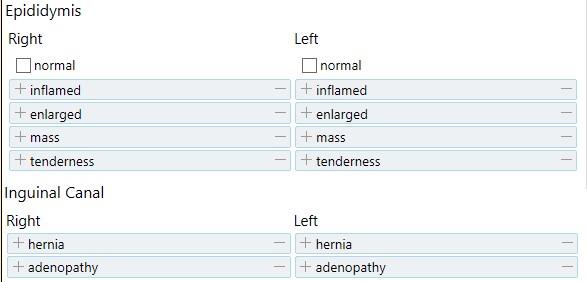
The Physical Exam
The full Physical Exam is divided into three parts: the General Exam, the Regional Exam, and the Special Exam. It serves to test the physiological functions of their body by using a variety of techniques and tools. These tools may include:| Age | (beats per minute) |
(breaths per minute) |
Blood Pressure |
|---|---|---|---|
| Premature | |||
| 0-3 months | |||
| 3-6 months | |||
| 6-12 months | |||
| 1-3 years | |||
| 3-6 years | |||
| 6-12 years | |||
| 13+ years |
| General | Head | Eyes | ENT | Cardiac |
|---|---|---|---|---|
| [ ] normal hygiene [ ] normal affect [ ] appears own age [ ] no acute distress |
[ ] no scars / bumps [ ] no deformities [ ] no trauma |
[ ] pupils equal / round [ ] reactive to light [ ] no icterus [ ] no conjunctival injection [ ] no papilledema |
[ ] normal hearing bilaterally [ ] no nasal discharge [ ] proper dentition [ ] moist mucous membranes [ ] no erythema [ ] no exudate [ ] no lymphadenopathy [ ] trachea midline |
[ ] regular rate / rhythm [ ] no murmurs / rubs / gallops [ ] normal distal pulses [ ] no JVD [ ] normal capillary refill [ ] no leg edema [ ] no varicose veins |
| Pulmonary | Abdominal | Genitourinary | Skin | Mental Status |
| [ ] normal tactile fremitus [ ] clear to percussion [ ] clear to auscultation [ ] normal bilateral entry / effort [ ] no wheezes / rales / rhonchi |
[ ] normal bowel sounds [ ] no aortic / renal bruits [ ] normal percussion [ ] abdomen soft / non-tender [ ] no distension / fluid [ ] no hepatomegaly [ ] no splenomegaly |
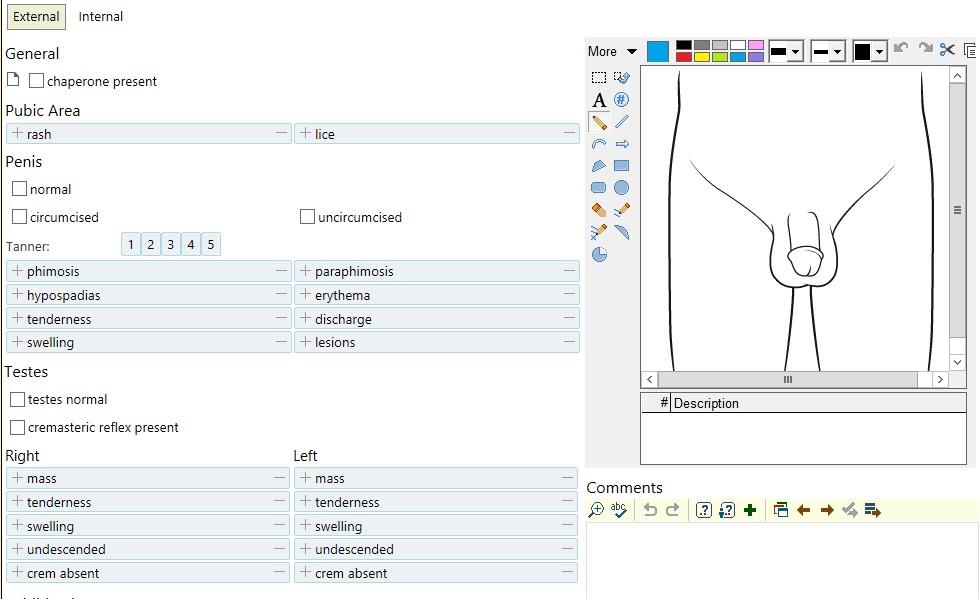
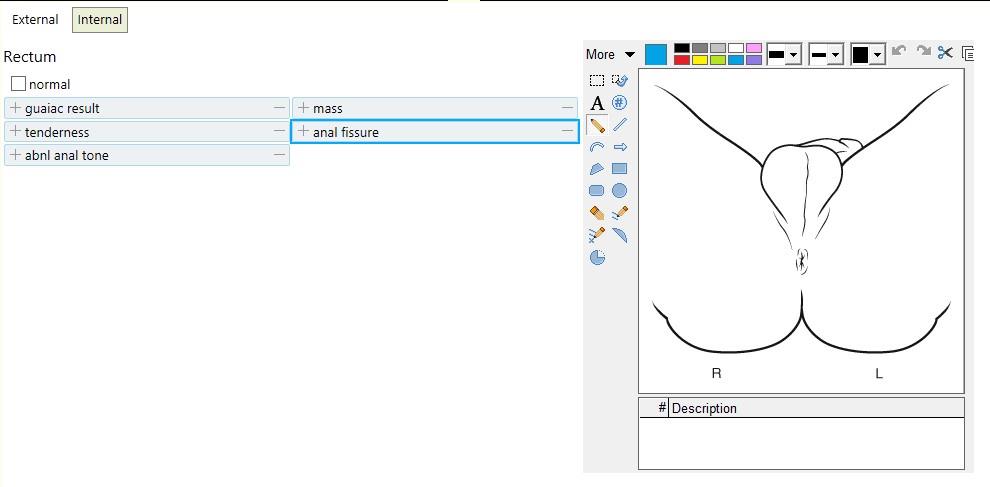
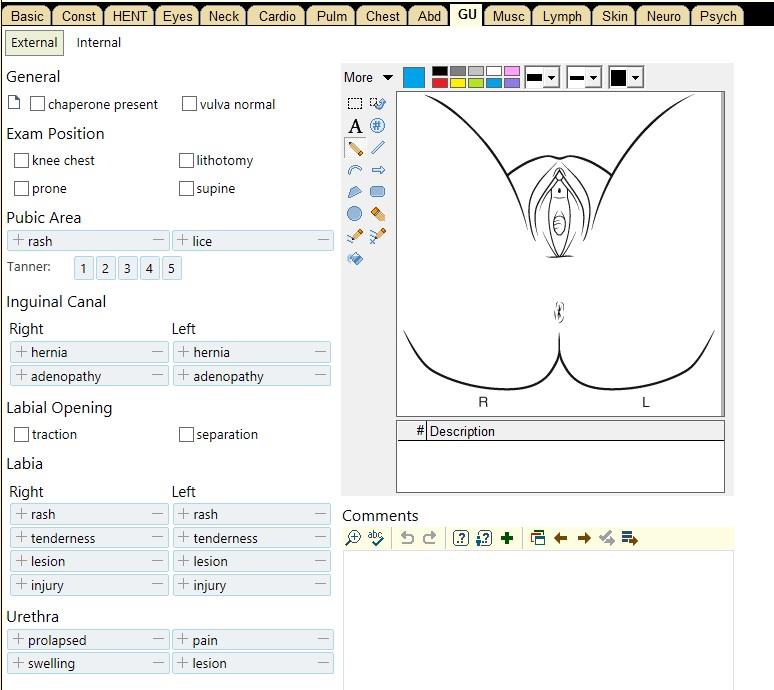
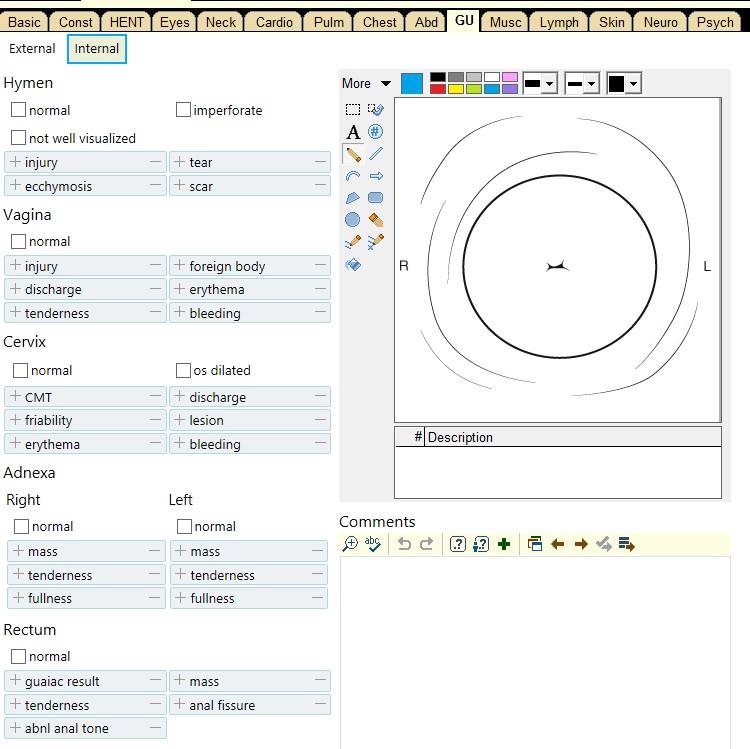
[ ] no hernias [ ] no cuts / lesions [ ] no rashes / ulcers [ ] no lymphadenopathy [ ] no discharge [ ] no bleeding [ ] no masses / induration Male: [ ] no scrotal masses [ ] no testicular swelling [ ] normal cremaster reflex Female: [ ] normal speculum exam [ ] normal bimanual exam |
[ ] no scars [ ] no rashes [ ] no bruises [ ] no masses |
[ ] awake [ ] alert [ ] oriented × _____/3 [ ] normal memory [ ] command following [ ] normal repetition [ ] no aphasia [ ] no dysarthria |
| Cranial Nerves | Strength | Reflexes | Sensation | Cerebellar |
| [ ] II: 20 / 20 visual acuity in both eyes, visual intact, and
primary pupillary reaction to light [ ] III, IV, and VI: EOMI, no nystagmus [ ] V: normal sensation, masseter and temporalis muscles intact [ ] VII: able to wrinkle forehead, smile, and close eyes normally [ ] VIII: hearing loss intact and equal bilaterally [ ] IX and X: palate rises equally, and uvula is midline [ ] XI: normal shoulder shrug and SCM muscle [ ] XII: tongue is midline and normal movements |
[ ] normal muscle tone / bulk [ ] normal range of motion upper extremity [ ] normal range of motion lower extremity [ ] no pronator drift _____/ S L upper extremity _____/ S R upper extremity _____/ S L lower extremity _____/ S R lower extremity |
Biceps L_____R_____ Triceps L_____R_____ Brachioradialis / Supinator L_____R_____ Patellar L_____R_____ Achilles L_____R_____ |
check pain, temperature, touch, and vibration upper proximal [ ] L [ ] R upper distal [ ] L [ ] R lower proximal [ ] L [ ] R lower distal [ ] L [ ] R |
[ ] normal finger to nose [ ] normal heel to shin [ ] normal gait [ ] tandem gait [ ] negative Romberg [ ] rapid alternating movements |
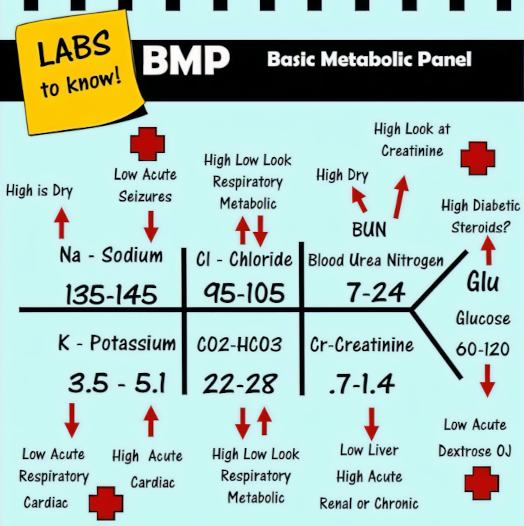
Diagnostics
After the Physical Exam, we come to the use of Labs and other diagnostic tools like Imaging. The purpose of diagnostic tests is to remove doubt and build a stronger case. We are trying to transform our provisional DDx into a final Diagnosis (Dx) in preparation for Treatment (Tx).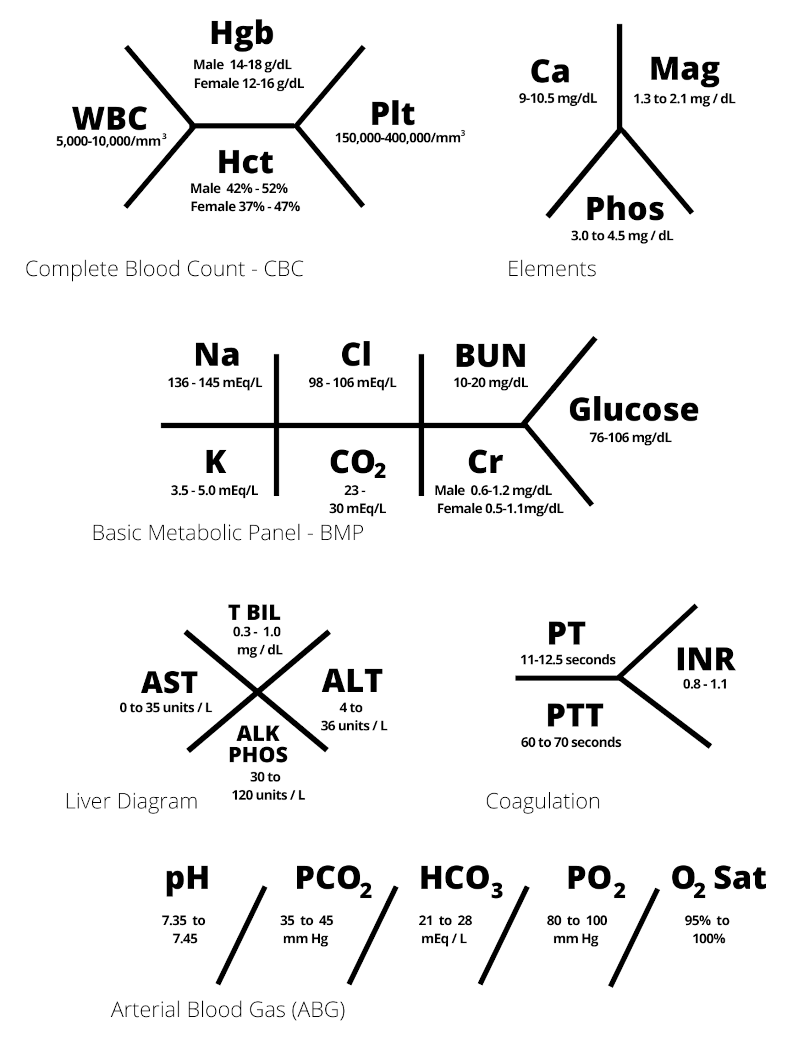
Final Assessment
After we have gathered as much information as we possibly can, we are finally ready to finalize our Dx. First, we might run through a broad overview of the different kinds of diseases that are possible in order to make sure that nothing has been forgotten or overlooked. This can be done by remembering our VITAMINS A, B, C, D, E, and K. While it is important to be properly nourished, we are not simply listing out the known vitamins. It is actually a mnemonic phrase for disease types [formulated by Zabidi A Zabidi-Hussin]:| Possible Causes | Comments |
|---|---|
| Vascular | Vessel (bleed or blocked); anything Hematology related |
| Infectious | includes post-infectious syndromes |
| Trauma | anything related to mechanical factors, like pressure or obstructions |
| Autoimmune / Allergy | |
| Metabolic | affecting aforementioned macromolecules and micronutrients |
| Idiopathic / Iatrogenic | of unknown origin or medically induced |
| Neoplasia | whether benign or malignant |
| Social | abuse, deprivation, etc. |
| Alcohol-related | |
| Behavioral | as in psychosomatic disorders |
| Congenital | present from birth |
| Degenerative or Drug-related | |
| Endocrine / Exocrine | |
| Karyotype | more specifically genetic in nature |
| Organ System or Problem | (click name for related calculator) |
Purpose | When To Use |
|---|---|---|---|
| Mental status assessment based on eye, verbal, and motor responses | With good reliability between observers, used for serial evaluation of mental status; also can be helpful for prognosis in certain conditions | ||
| Quantifies severity of stroke in acute setting based on physical findings alone | Use in acute setting to determine severity and estimates long-term prognosis after an acute stroke | ||
| Estimates stroke risk for patients with atrial fibrillation and suggests need for pharmacotherapy | To risk stratify patients with atrial fibrillation by risk of stroke and to guide the decision to start anticoagulation. Helpful to compare to HAS-BLED score (see below) | ||
| Estimates 10-year risk of myocardial infarction (MI) or coronary death in individuals without prior heart disease, intermittent claudication, or diabetes | Used to estimate 10-year risk for MI/death for patients without previous cardiac events; can be helpful in the management of hyperlipidemia and in assessing if primary prevention with aspirin would have benefit | ||
| Estimates risk of major bleeding for patients with atrial fibrillation on anti-coagulation | In concert with CHA2DS2-VASc, used to guide the decision to start anti-coagulation in patients with atrial fibrillation | ||
| Estimates 6-week risk of major adverse cardiac events in patients ≥ 21 years-old presenting with symptoms suggesting acute coronary syndrome | To guide decision in emergency department if patients can be discharged or if need additional testing or admission by stratifying patients into low, moderate, and high-risk groups | ||
| Estimates 30-day risk of death, MI, or cardiac arrest after non-cardiac surgery | To help risk stratify patients prior to surgery and to allow for shared decision making, especially in those with additional risk factors | ||
| Estimates 30-day mortality risk in patients with acute coronary syndrome based on age, blood pressure, and heart rate | Use to risk stratify patients and guide initial therapy | ||
| Estimates risk of DVT in patients, particularly in emergency and outpatient settings | Use to exclude need for lower extremity duplex ultrasound in low risk patients | ||
| Estimates risk of PE to be < 2% when all criteria are negative and pre-test probability is low (< 15%) | To rule out need for additional testing for PE based on clinical criteria alone | ||
| Estimates risk of PE in emergency department settings | To risk stratify patients and exclude need for additional testing such as a CT angiogram in low risk patients | ||
| Estimates prognosis of patients with cirrhosis and approximates abdominal surgery peri-operative mortality | Used to determine prognosis and in listing for transplantation | ||
| Estimates short term prognosis in patients with alcoholic hepatitis and benefit of steroid therapy | To evaluate severity of alcoholic hepatitis and guide decision on steroid administration | ||
| Estimates 3-month mortality in patients > 12 years old with end-stage liver disease | For stratification of patients for liver transplantation and prediction of mortality in specific clinical scenarios, such as non-transplantation surgeries | ||
| Classifies severity of acute kidney injury by GFR and urine output | To determine severity and prognosis of acute kidney injury | ||
| Estimates probability of strep pharyngitis in acute pharyngitis of < 3 days onset and recommends next steps | To determine need for testing and empiric antibiotic treatment for acute pharyngitis secondary to Streptococcal pyogenes | ||
| Estimates 30-day mortality of community-acquired pneumonia | To help determine if patients can be treated outpatient versus inpatient, with consideration for ICU admission | ||
| Predicts risk of mortality in hospitalized patients with suspected infection outside of the intensive care unit based on bedside findings | Use at the bedside to prompt additional monitoring,testing, and/or treatment of patients with possible severe infections (sepsis) | ||
| To classify infection status in patients with suspicion of SIRS, sepsis, or septic shock | Used as a screening or triage tool to identify patients who may need to be initiated on a sepsis protocol | ||
Treatment Plan (Present & Future)
As per the Hippocratic Oath, one should always genuinely try to "do no harm." Therefore, choices are always made with consideration for, and the consent of, the person. This includes everything that would normally be covered within the concept of Person-Centered Care.
| Alert |
| responding to Verbal stimuli |
| responding to Painful stimuli |
| Unconscious |
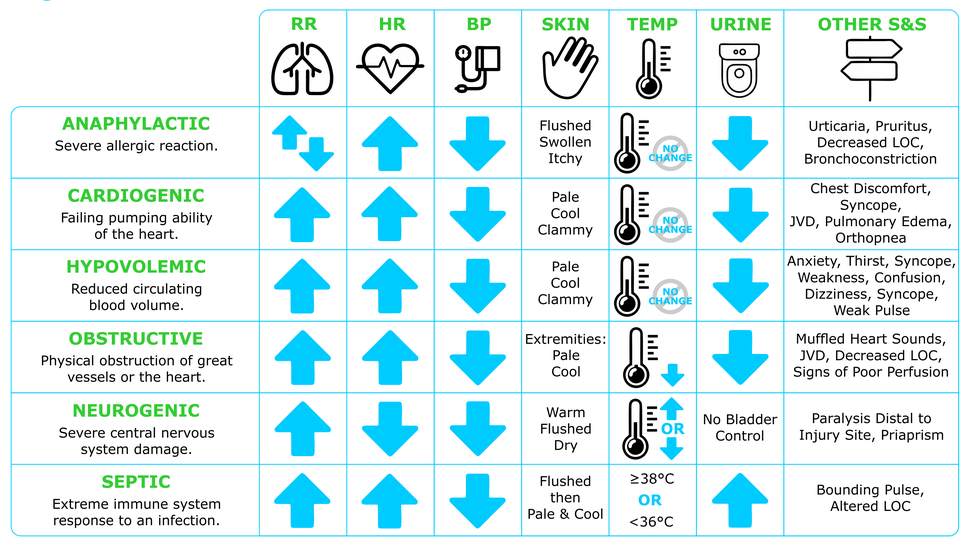
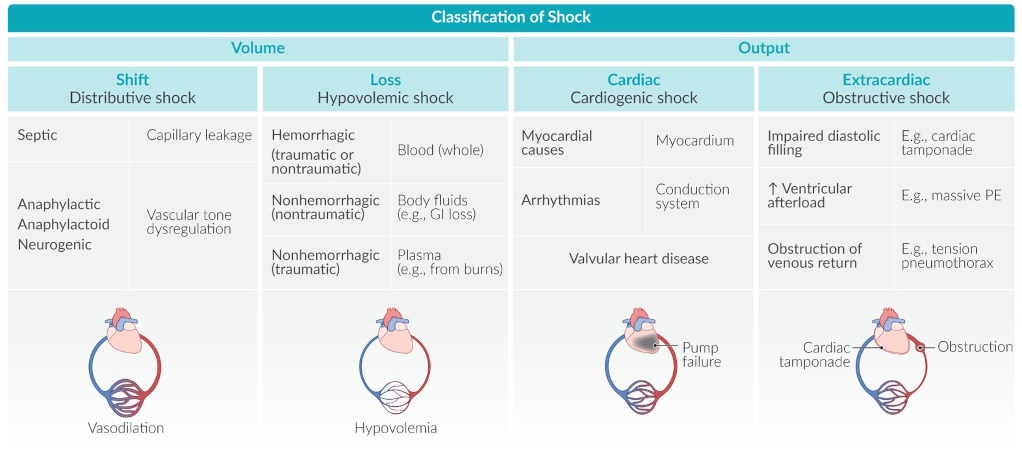
| Shock Type | Plumbing Analogy | Examples |
|---|---|---|
| "pipe problem" | During anaphylaxis, the blood vessels rapidly dilate and blood pressure drops; notice the similarities to an immune response during sepsis; most common type of shock (~66% of cases) | |
| "fluid problem" | Bleeding out from a hemorrhage, whether internally or externally; lacking sodium and water due to dehydration from excess vomiting, diarrhea, or sweating like in foodborne illnesses or heat stroke | |
| "pump problem" | Heart failure from Myocardial Infarction (MI), mechanical rupture, etc. | |
| "plug / pressure problem" | A block in the artery of a lung, Pulmonary Embolism (PE); air trapped within the pleural space causing pressure between lung and chest wall, Pneumothorax |


Medical Records
All diagnoses and treatments will be recorded in some form (for future reference, for billing, for legal reasons, for research, etc.). Part of this process may require us to write a "SOAP note." This stands for Subjective, Objective, Assessment, and Plan. We already have an idea of what to put within each section.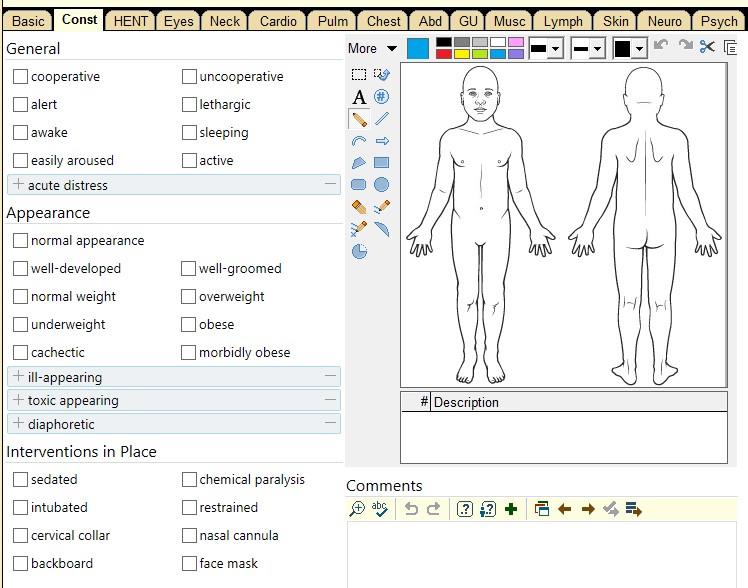
Hospital Structure
The more that I learn of medical education and the structure of most hospitals, the more that I can see why the healthcare system is so broken. That is not a criticism of the people involved. There are many good healthcare providers, people who are kind, considerate, humble, and hard-working. But they are good in spite of it, not because of it. Please do not lose the sensitivity that God has placed within your heart as you engage with it.
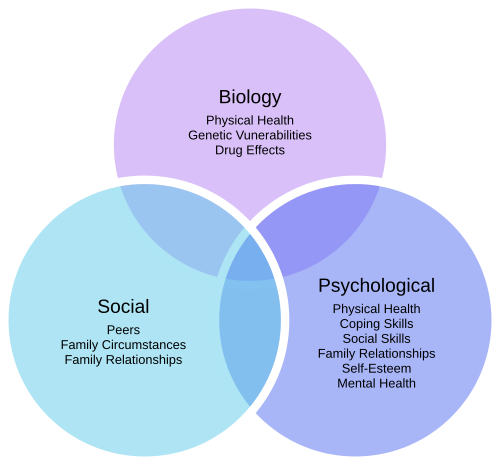
...So, the major critique of the Medicine, the dominant Medicine, was that it separates the body from the psyche, the somatic from the psychology. It separates the person from its environment. It doesn't take into consideration the relation between the doctor and the patient. And most of all, it divides the body, the organism, into parts and doesn't connect them again. It loses everything that has to do with the totality of the organism...In practice, this resulted in patients initially meeting with three different types of healthcare providers as a group: a general practitioner, a psychiatrist/psychologist, and a social worker. There is already research on the effectiveness of combining GPs and psychiatrists, as well as GPs and social workers. By having multiple specialists working together simultaneously, many benefits are possible. For example, a social worker could help a patient draw up an Ecomap to help them to understand the support system that they can rely on as they heal from the physical treatment provided by a GP, while a psychologist can give them strategies to cope with any anxiety that they might be feeling about it.
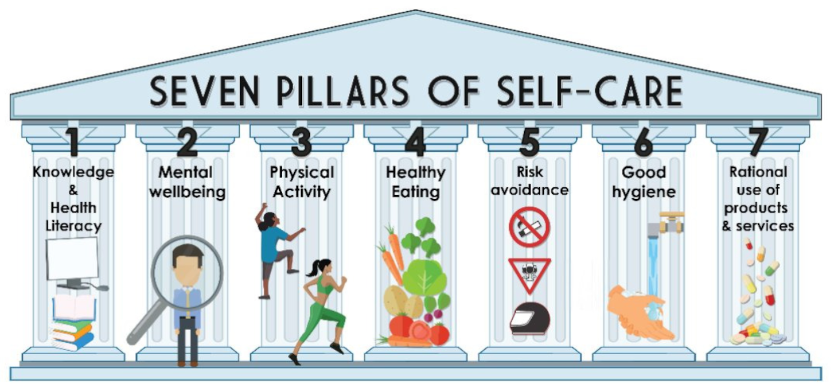
Self-Care and The Heart of a Healer
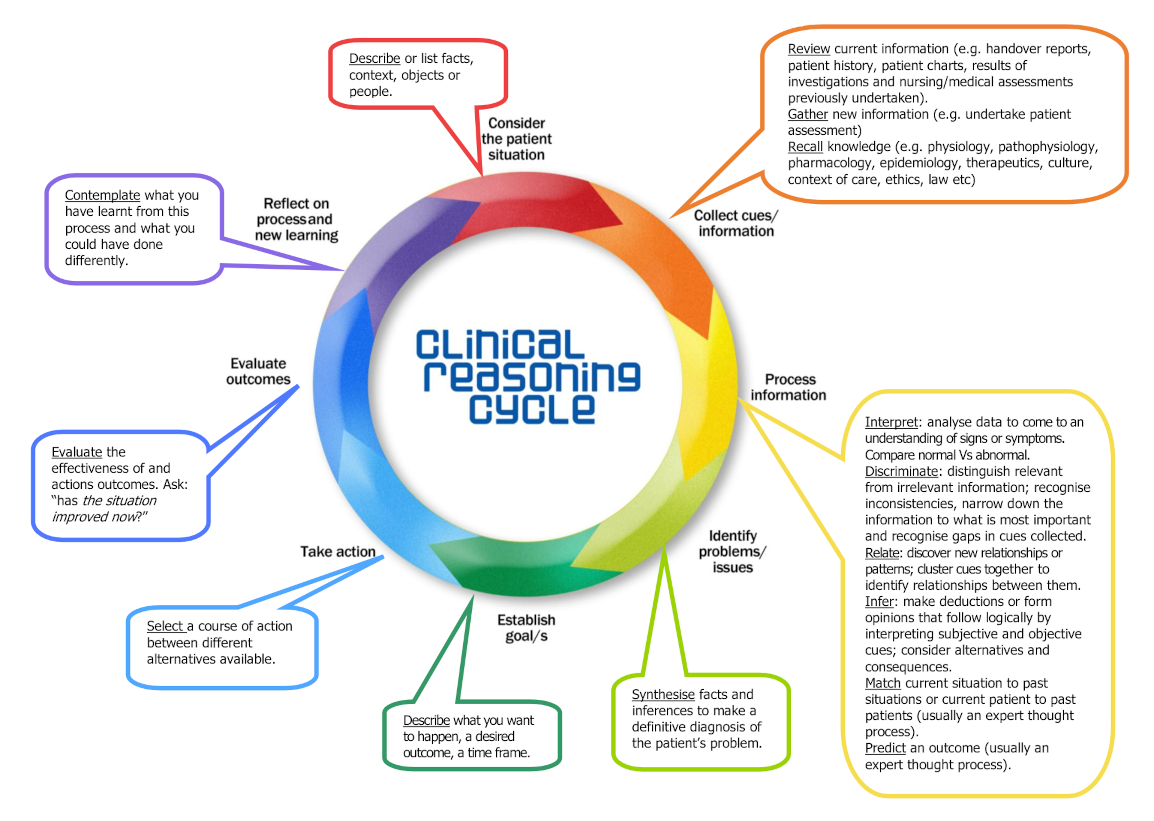
Many people who become a part of healthcare do so because they genuinely want to help others. However, being repeatedly exposed to other's pains can lead to vicarious trauma, and eventually, to compassion fatigue. In other words, one can deal with other's trauma so much that they become traumatized themselves and somewhat apathetic as a result.| Step | Description | Example Scenario |
|---|---|---|
| Describe or list facts, context, objects, or people | • This 60 year old patient is in ICU because he had an abdominal aortic aneurysm (AAA) surgery yesterday | |
| Review current information (e.g.: handover reports, patient history, patient charts, results of investigations and nursing/medical assessments previously undertaken) | • He has a history of hypertension and he takes betablockers • His BP was 140/80 an hour ago |
|
| Gather new information (e.g.: undertake patient assessment) | • I've checked his BP and it is now 110/60 • Temperature 38 degrees • Epidural running @ 10ml/hr |
|
| Recall knowledge (e.g. physiology, pathophysiology, pharmacology, epidemiology, therapeutics, culture, context of care, ethics, law, etc.) | • BP is related to fluid status • Epidurals can drop the BP because they cause vasodilation • In ICU, we have standing orders for epidural management |
|
| Interpret: analyze data to come to an understanding of signs or symptoms; compare normal vs. abnormal | • His BP is low, especially for a person who is normally hypertensive | |
| Discriminate: distinguish relevant from irrelevant information; recognize inconsistencies, narrow down the information to what is most important, and recognize gaps in cues collected | • His temp is up a bit, but I'm not too worried about it - I'm more concerned about his BP and pulse • I'd better check his urine output and his O2 sats |
|
| Relate: discover new relationships or patterns; cluster cues together to identify relationships between them | • His hypotension, tachycardia, and oliguria could be signs of impending shock • His BP went down after we increased the epidural |
|
| Infer: make deductions or form opinions that follow logically by interpreting subjective and objective cues; consider alternatives and consequences | • His BP could be low because of blood loss during surgery or because of the epidural | |
| Match current situation to past situations or current patient to past patients (usually an expert thought process) | • AAAs often have hypotension post op | |
| Predict an outcome (usually an expert thought process) | • If I don't give him more fluids he could go into shock | |
| Synthesize facts and inferences to make a definitive diagnosis of the patient's problem | • He is hypovolemic and the epidural has worsened the BP by causing vasodilation | |
| Describe what you want to happen, a desired outcome, a time frame | • I want to improve his hemodynamic status - get his BP up and urine output back to normal over the next hour | |
| Select a course of action between different alternatives available | • I will call the doctor to get an order to increase his IV rate and to give Metaraminol if needed | |
| Evaluate the effectiveness of outcomes and actions; ask: "Has the situation improved now?" | • His BP is up for now but we will need to keep an eye on it as he may still need Metaraminol a bit later; his urine output is averaging > 30mL/hr now | |
| Contemplate what you have learned from this process and what you could have done differently | • Next time I would... • I should have... • If I had... • I now understand... |
|
| Characteristic | Description |
|---|---|
| Confidence | Assurance of one's reasoning abilities |
| Contextual Perspective | Considerate of the whole situation, including relationships, background, situation, and environment |
| Creativity | Intellectual inquisitiveness used to generate, discover, or restructure ideas; the ability to imagine alternatives |
| Flexibility | Capacity to adapt, accommodate, modify or change thoughts, ideas, and behaviors |
| Inquisitiveness | Eagerness to learn by seeking knowledge and understanding through observation and thoughtful questioning in order to explore possibilities and alternatives |
| Intellectual Integrity | Seeking the truth through sincere, honest processes, even if the results are contrary to one's assumptions or beliefs |
| Intuition | Insightful patterns of knowing brought about by previous experience and pattern recognition |
| Open-Mindedness | Receptiveness to divergent views and sensitivity to one's biases, preconceptions, assumptions, and stereotypes |
| Perseverance | Pursuit of learning and determination to overcome obstacles |
| Reflective | Contemplation of assumptions, thinking and action for the purpose of deeper understanding and self-evaluation |
